
A. Sleep Needs, Stress, and Sleep Loss
“Sleep is vital to your well-being, as important as the air you breathe, the water you drink and the food you eat.” (219)—National Sleep Foundation.
Animal studies have demonstrated that sleep properly belongs in Maslow’s hierarchy of needs as indispensable to survival. (191, 192) Sleep is “not some biological luxury.” (220) “Sleep is biologically obligatory.” (5) Animals deprived of sleep die. (191, 220, 221)
 “[T]he sleep-wake cycle is intrinsic and inevitable, not a pattern to which people voluntarily adhere or can decide to ignore. Despite the tendency of society today to give sleep less priority than other activities, sleepiness and performance impairment are neurobiological responses of the human brain to sleep deprivation. Training, occupation, education, motivation, skill level, and intelligence exert no influence on reducing the need for sleep. Micro-sleeps, or involuntary intrusions of sleep or near sleep, can overcome the best intentions to remain awake.” (222)
“[T]he sleep-wake cycle is intrinsic and inevitable, not a pattern to which people voluntarily adhere or can decide to ignore. Despite the tendency of society today to give sleep less priority than other activities, sleepiness and performance impairment are neurobiological responses of the human brain to sleep deprivation. Training, occupation, education, motivation, skill level, and intelligence exert no influence on reducing the need for sleep. Micro-sleeps, or involuntary intrusions of sleep or near sleep, can overcome the best intentions to remain awake.” (222)
A recent Australian study, (223) though rather fiercely challenged, (224) suggests further research is needed to properly determine children’s sleep requirements. (223) Australian scientists observe that the recommendation of 9.25 hours for adolescents (5) was initially based on findings from a “single classic study conducted by Carskadon and colleagues (Carskadon, Keenan and Dement 1987)” at Stanford University between 1975 and 1985. (147)
“As part of the longitudinal study, children, aged 10 to 17 years, returned to sleep camp each summer with the total amount of time in bed held constant each year. Sleep ‘need’ was operationally defined as the amount of sleep obtained in the sleep opportunities for each assessment (Carskadon et al. 2002). The study found that total nocturnal sleep length remained unchanged at about 9.25 hours across the adolescent span when adolescents were provided a 10-hour sleep opportunity, and sleep was not constrained to their habitual schedule (Carskadon 1982; Carskadon et al. 2002). [¶] Although participants were asked to maintain the scheduled study bed times for 10 days prior to each session, sleep diaries generally revealed that the children, particularly the older adolescents, failed to comply (Carskadon et al. 1983). Thus, defining adolescent sleep ‘need’ as the amount of sleep obtained in the sleep opportunities provided (Carskadon et al. 2002) may have yielded inaccurate results or influenced the conclusions drawn. It may be more accurate to interpret adolescents sleep durations as an interaction between their basal sleep need and their accumulated sleep debt.” (147)
In 2016, Canadian researchers echoed their Australian counterparts’ sentiments, declaring that “the best available evidence that can inform the sleep duration recommendations is weak, suggesting that expert opinion is needed until we have more research.” (224.5) Notwithstanding these critiques, “[t]here is a general consensus among sleep researchers that adolescents require approximately 9 to 10 hours of sleep per night for optimal functioning in a number of domains including school performance, mood regulation, ![]() cognitive processes including reaction speed and attention, and overall health[.]” (225.5) In a recent study, CDC scientists utilized National Sleep Foundation standards for adolescents; i.e., sleep is insufficient if <8 hours per night, borderline if 8 hours per night, and optimal if >9 hours per night. (26) Relying upon National Heart, Lung, and Blood Institute guidelines, the CDC website advises that teenagers require 9-10 hours of sleep per night. (225.7) In its 2014 secondary school start time Policy Statement, the American Academy of Pediatrics identifies 8.5-9.5 hours of sleep as “optimal” for adolescents. (54) Professors Carskadon and Wolfson, noted among the Policy Statement’s contributing authors, (54) previously pointed to ~9.2 hours of sleep as “optimal” and ~8.5 hours as “adequate” for this population. (12)
cognitive processes including reaction speed and attention, and overall health[.]” (225.5) In a recent study, CDC scientists utilized National Sleep Foundation standards for adolescents; i.e., sleep is insufficient if <8 hours per night, borderline if 8 hours per night, and optimal if >9 hours per night. (26) Relying upon National Heart, Lung, and Blood Institute guidelines, the CDC website advises that teenagers require 9-10 hours of sleep per night. (225.7) In its 2014 secondary school start time Policy Statement, the American Academy of Pediatrics identifies 8.5-9.5 hours of sleep as “optimal” for adolescents. (54) Professors Carskadon and Wolfson, noted among the Policy Statement’s contributing authors, (54) previously pointed to ~9.2 hours of sleep as “optimal” and ~8.5 hours as “adequate” for this population. (12) 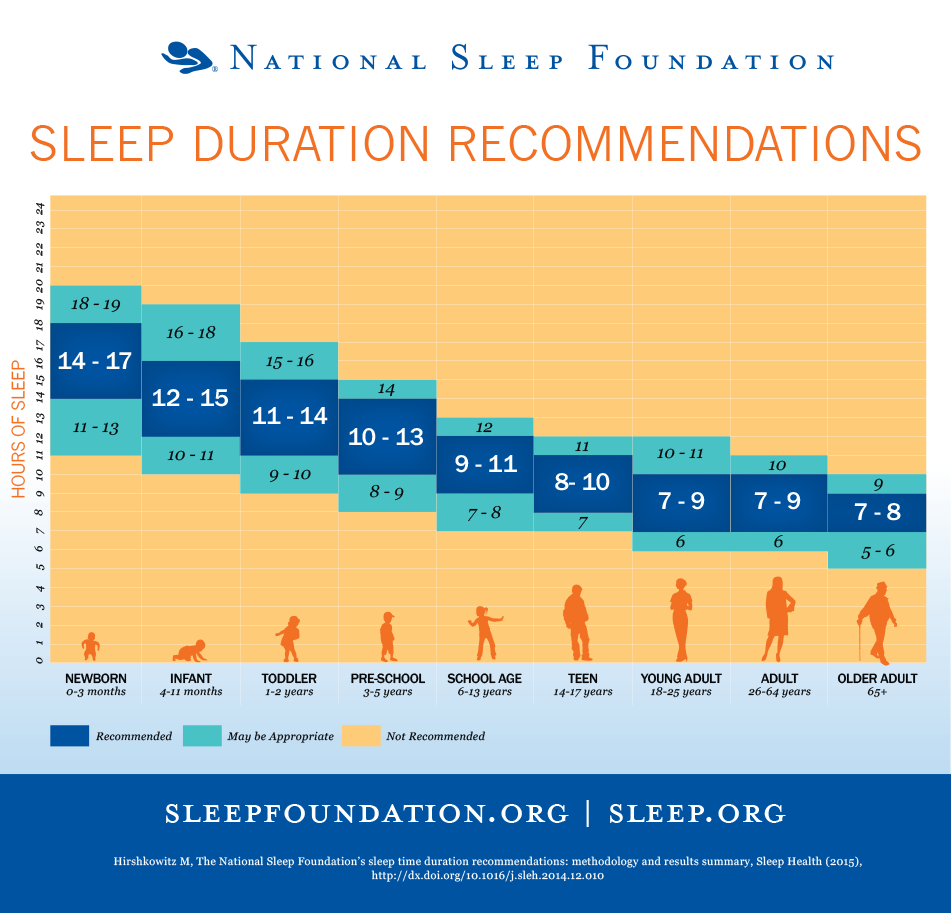
In 2015, the National Sleep Foundation reviewed and revised its previous sleep duration recommendations, now advising that children 9 to 13 years of age need 9-11 hours of sleep per night, though as few as 7-8 hours and as many as 12 hours may be appropriate. (9.5) Teenagers 14-17 years of age are said to require 8-10 hours of sleep per night, though as few as 7 hours and as many as 11 hours may be appropriate. (9.5) In 2016, the American Academy of Sleep Medicine released its consensus sleep duration recommendations, proposing that “to promote optimal health[,]” children 6 to 12 years of age should sleep 9 to 12 hours nightly, and teenagers 13 to 18 years of age should sleep 8 to 10 hours nightly. (9.7)
Survey studies regularly find adolescents desire more sleep than they obtain. (1.5, 147)
“Consistent with laboratory data, the self-reported sleep need of adolescents is frequently greater than 9 hours, indicating a disparity between what adolescents say they need and what they actually obtain. In a large survey study (Wolfson, et al. 1998) that examined the sleep patterns and preferences of American adolescents, approximately 87% of adolescents reported needing more sleep than they obtained on weeknights. Those who indicated needing more sleep reported an ideal sleep time of nine hours, about two hours more than they were getting. Similarly, adolescents in Germany (Mercer, Merritt and Cowell 1998) stated their subjective sleep need to be around nine hours. Several other studies have also found that adolescents frequently report their sleep time to be insufficient (Lazaratou, Dikeos, Anagnostopoulos, Sbokou and Soldatos 2005) and endorse a wish for sleep (Strauch et al. 1988).” (147)
 Early sleep research suggested that after birth, sleep requirements declined during childhood development, leveling off at eight hours during puberty. (2) Research over the past thirty years, however, has demonstrated that the number of sleep hours required during the “explosion of growth and other body changes of puberty” may be nine hours or more throughout adolescence. (2)
Early sleep research suggested that after birth, sleep requirements declined during childhood development, leveling off at eight hours during puberty. (2) Research over the past thirty years, however, has demonstrated that the number of sleep hours required during the “explosion of growth and other body changes of puberty” may be nine hours or more throughout adolescence. (2)
“Mere rest does not create the restorative state of having slept. [¶] The fundamental difference between sleep and a deeply relaxed wakefulness is that sleep involves dropping into a state with a relative loss of awareness of and responsiveness to the external world. This state of unresponsiveness appears to be necessary for the restorative processes that occur during sleep to take place.” (220, italics in original.)
“Sleep … helps to restore both mind and body. The body’s engines are able to slow down and cool off when we sleep, decreasing the metabolic processes, heart rate, respiration, digestion, and body temperature. Sleep can also be a time of increased healing or, in children, a time of accelerated growth.” (Abaci, Take Charge of Your Chronic Pain: The Latest Research, Cutting-Edge Tools (Globe Pequot Press 2010) p. 241, n. omitted.) Deep sleep coincides with the release of growth hormone in children and young adults. (192) “[S]leep seems to be particularly important during periods of brain maturation. (Across species, maturing individuals sleep more than fully mature individuals.)” (220)
“Given the vital importance of sleep, it can be concluded that adolescence is a critical period for normal growth and development in which sleep, in a complex association with many other processes, plays an important role. [¶] Sleep architecture is vulnerable to a complex interaction between maturational, situational, and pathological changes in sleep during this period.” (221)
 Restricted sleep and interrupted circadian timing (see, §§ II, supra; II.B., III, et seq., infra), serve as environmental/physiological stressors in humans. (183, 226, Wise, Hopkin, & Garland, Handbook of Aviation Human Factors (CRC Press 2nd ed. 2009) p. 18-3.) Sleep loss means sustaining wakefulness longer, which stresses the body, leading to “additional problems.” (228) “[A]dolescent sleep systems appear to become more vulnerable to stress at a time when social turmoil and difficulties are often increasing.” (220) George Chrousos, M.D., Professor and Chairman Department of Pediatrics at Athens University Medical School, advises:
Restricted sleep and interrupted circadian timing (see, §§ II, supra; II.B., III, et seq., infra), serve as environmental/physiological stressors in humans. (183, 226, Wise, Hopkin, & Garland, Handbook of Aviation Human Factors (CRC Press 2nd ed. 2009) p. 18-3.) Sleep loss means sustaining wakefulness longer, which stresses the body, leading to “additional problems.” (228) “[A]dolescent sleep systems appear to become more vulnerable to stress at a time when social turmoil and difficulties are often increasing.” (220) George Chrousos, M.D., Professor and Chairman Department of Pediatrics at Athens University Medical School, advises:
“Prenatal development, infancy, childhood and adolescence are times of increased vulnerability to stressors. The presence of stressors during these critical periods can have prolonged effects, such as sustained cacostasis [defective homeostasis, dyshomeostasis, distress] that can last the entire lifetime of an individual.” (227)
A recent study by University of Cincinnati Professor of Sociology David Maume, Ph.D., finds “stressful social ties disrupt youths’ sleep, as when family composition changes because of divorce or remarriage, families live closer to poverty, or schools pile on the homework. On the other hand, youths had healthier sleep (longer duration and of higher quality) when social ties were a source of support, such as when they felt part of the schools they attended or they were surrounded by academically oriented and prosocial friends. [I]t is not any one social tie but rather the ‘constellation of social ties [that] matters most for health habits in adolescents.’” (229)
 Students from lower socioeconomic backgrounds have a “higher probability of exposure to adverse, unstable conditions that may potentially affect sleep.” (Wolfson & Richards, Young Adolescents: Struggles with Insufficient Sleep, publish. in, Sleep and Development (Oxford Univ. Press, El Sheikh edit. 2011) p. 272, citations omitted.) According to the National Center for Education Statistics, in 2012, approximately 21 percent of U.S. children aged 5-17 were living in poverty, ranging from 11 percent in North Dakota to 32 percent in Mississippi. (230) As University of California Professor of Community Health and Human Development Ronald Dahl, M.D., explains, “sleep is naturally restricted to times and places that feel safe.” (220)
Students from lower socioeconomic backgrounds have a “higher probability of exposure to adverse, unstable conditions that may potentially affect sleep.” (Wolfson & Richards, Young Adolescents: Struggles with Insufficient Sleep, publish. in, Sleep and Development (Oxford Univ. Press, El Sheikh edit. 2011) p. 272, citations omitted.) According to the National Center for Education Statistics, in 2012, approximately 21 percent of U.S. children aged 5-17 were living in poverty, ranging from 11 percent in North Dakota to 32 percent in Mississippi. (230) As University of California Professor of Community Health and Human Development Ronald Dahl, M.D., explains, “sleep is naturally restricted to times and places that feel safe.” (220)
“Most species have evolved mechanisms to ensure that sleep is limited to such safe places as burrows and nests and to times of relative safety from predators. In humans, there is a similar tendency for safe feelings to promote sleep while feelings of threat or stress tend to inhibit sleep. [¶] These links between sleep and stress are an important source of sleep disruption among adolescents. A key point can be best illustrated by a brief consideration of the evolutionary underpinnings of these biological links between sleep and emotion. For most of early human history, large nocturnal-hunting carnivores surrounded our ancestors, who had no access to  physically safe sleep sites. (Humans cannot sleep in trees or on cliff edges, because we lose all muscle tone during REM sleep.) In the human ancestral environment, the main protection against predators was a close-knit social group. The human brain evolved under conditions that made this sense of social belonging and social connectedness the basis for feelings of relative safety. Natural tendencies in the human brain continue to reflect these links, so that fears of social rejection can evoke powerful feelings of threat and so lead to sleep disruption, while feelings of love, caring, and social connection create a feeling of safety and so promote sleep.” (220)
physically safe sleep sites. (Humans cannot sleep in trees or on cliff edges, because we lose all muscle tone during REM sleep.) In the human ancestral environment, the main protection against predators was a close-knit social group. The human brain evolved under conditions that made this sense of social belonging and social connectedness the basis for feelings of relative safety. Natural tendencies in the human brain continue to reflect these links, so that fears of social rejection can evoke powerful feelings of threat and so lead to sleep disruption, while feelings of love, caring, and social connection create a feeling of safety and so promote sleep.” (220)
